“Colin Griffin has no regrets about taking a step back from his athletics career last month. But now he hopes the sport can take a giant leap forward in how it deals with elite competitors.
On the way to meet you, he got a call from a friend. They talk most days, like you may do with your best friend, only yours isn’t a world champion. Colin Griffin’s is.
For more than a decade now Rob Heffernan has been a contemporary, something of a rival but mostly a friend. When either of them was struggling, the other was there to hear and help the other out.
When Heffernan awoke the morning of the 2012 Olympics 50km race, Griffin was in the other bed, his roommate for most major championships.
Yet when Heffernan finally had his moment in time last August, shuffling into that stadium in Moscow and grinning over the finishing line, Griffin wasn’t there.
Instead, he was back home, in a Dublin apartment, on Twitter like some kind of parachuted commentator explaining to half the country the nuances of just how his old friend had won.
He won’t lie, it was a surreal experience: Rob finally winning a big one and him on a sofa back home. He was delighted for Heffernan and was there at the airport to greet him upon his return, but while he hoped it ignited droves of kids and athletes to take up or step up in the sport and event he loves, it didn’t spark anything in him to give it another go.
The year 2013 had been one of the most testings in a very testing career. Too much time was spent challenging administrators rather than fellow competitors on the road. The week before Christmas he announced his decision: he was putting his athletic career on hold. At 31 he was still too young to close the door on an event that favours the older athlete, but he couldn’t keep putting the rest of his life on pause either.
“Being a full-time athlete for all those years is an intense lifestyle. When things go well and you make a breakthrough it’s brilliant, you experience this euphoric feeling. When things don’t go well you are challenged.
“I’ve probably had more of those challenging moments than those euphoric moments, especially in the last couple of years. And that does take its toll. There are only so many times you can put yourself out there.
“The reality is very few athletes make a living out of the sport. Even major championship winners like Rob and Derval [O’Rourke] have no guarantees and little security, so someone like myself further down the chain can only do it for so many years. It’s like, I love this sport but can I really keep justifying doing 200km a week and all those hours training in something that doesn’t bring in a sustainable income?
“I’m 31, in a long-term relationship and you want to be thinking ahead. I didn’t want to be 35 with no pension fund or real experience in a career outside athletes.
“I didn’t want to close the door on competing for good and then have regrets in 10 years’ time, but I want to get my business developed. That’s going to be a 24/7 job. So is being an international athlete so putting the two together is just not feasible.”
We’re talking in a café on Canal Dock in Dublin. He’s from Leitrim, then studied and trained in Limerick for years but moved to the capital last year just like his Belfast-born girlfriend, Clare, did as well. This is where he plans to have his own business: an altitude training gym in the biggest population centre in the country.
He’s been working on the side in that area for a few years now but after the Olympics and the ordeal of last year, it’s athletics that he’s now pushed to the margins.
You may well not know what happened to Colin Griffin in London, how hard it was for him to make it there in the first place. Or maybe you do and have had a cursory look at his career. Constantly being disqualified in races because of a questionable technique, including London. Appealed a decision by the chief of Athletics Ireland that he shouldn’t receive any Sports Council funding. Just yesterday in the Irish Examiner pronouncing athletes should have their own representative body along the lines of the GPA.
And from that remove maybe you’ve come to some conclusions. That he’s an agitator. Too opinionated, too old, too limited and too much hassle to invest in or care about.
It’s not like that though. He’s opinionated alright, but it’s always a cool, calculated, rational, sober view he offers, without a hint of the chippiness or outrage or sarcasm.
So when he says that Irish athletes should have a GPA-like service, that Irish athletics doesn’t respect its coaches or athletes enough, that there should be a national head coach for each athletic discipline, it’s worth listening to. He may be no Keane or Derval or Rob Heffernan but he’s experienced, intelligent, insightful and sensible. He’s learned a lot from his career in athletics. Athletics, and not just athletes, have a lot to learn from him.
London was supposed to the pinnacle of that career in athletics. And it so nearly was. Once he qualified for it at the last possible attempt in a race in a Russian town called Saransk, he promised to enjoy the lead up as well as train hard. He did both and when he and Heffernan awoke that morning of Saturday, August 11, he felt it was going to be his day of days. Laura Reynolds, whom he coaches, was competing later that afternoon in the women’s 20k. It was his parents’ wedding anniversary. Speckled everywhere along the route were well-wishers from Ireland. “Up Leitrim!” “Go on, Colin!” ‘Come on, Ireland!” There were goodwill and energy everywhere.
At 25k he picked up his first red card, and then at 35k when he lost a group, he picked up a second, his unorthodox technique all the more conspicuous due to his isolation and height. Walking is a bit like baseball – three strikes and you’re out – but when Griffin rejoined a group that were all vying for a top-16 spot, he was back on track.
“I was attacking the race like this was what I always wanted. I was on the course for time five minutes better than my personal best. I was having the race of my life.”
And then just like that, it was all over. At the 38km mark, he looked up at the big screen and saw the third dot alongside his name. A judge stepped out to confirm that once again he didn’t have one of his feet in contact with the ground. It didn’t matter that it was only a judge’s opinion; in walking, a judge is a judge.
The rest of the day was a mix of emotions. He gathered and braced himself for the awaiting media. He urged Rob Heffernan on. Then from the drinks table, he would urge Laura on to a top-20 finish, a remarkable achievement for an athlete of her inexperience. The next morning it hit him. He didn’t know if he wanted to compete at this level anymore.
A few months later he and Clare headed off to Australia to help clear his head. If anything it became more confused over there. The day they arrived he received an email from Athletics Ireland high-performance director Kevin Ankrom, informing him he wasn’t going to be forwarded for any Sports Council funding for 2013.
“I met the criteria for that year. So while I understood he was entitled to his recommendation and that I had no automatic entitlement to be carded, I felt I at least should have a chance to appeal. I mailed him back but didn’t hear anything for another month until the Sports Council deadline had passed. I was top 16 in the world. I met the A standard. Yes, I was disqualified at the Olympics but I had qualified for the Olympics (without any funding in 2012) and felt with the right support I was capable of a big performance on any given day. I felt the glass was half full rather than half empty, whereas instead I was perceived as a liability, not worthy of investing in.
“That’s the way they put it: you’ve received a cumulative €90,000 in funding since 1999 and the investment isn’t working out. I would say to that I’ve learned a lot over those 13 years. I’ve become a coach. I’ve been able to bring altitude training back to Ireland and while I’ll hardly transform the economy I will be creating employment. All these little things add up as value for the taxpayers’ money. But they don’t see value in that.”
One member on the Athletics Ireland board did. Liam Moggan agreed that Griffin was entitled to an appeal process and after much wrangling, he was granted one in April. It was recommended that he should receive a grant of €6,000 for the year but even after Ankrom and Griffin shook on that there would be disputes about how it was distributed. In July Griffin called Ankrom to inform him of his displeasure, and as he puts it, “the conversation was less than friendly”.
For Griffin that was his breaking point, not London. Last March after he’d returned from Australia he’d returned to London for a few days, strolled around The Mall and Constitution Hill which the 50km walk route took in. He also popped over to Strafford where the Olympic park and village had been. Now it was like they had never been there. London had moved on from the Olympics. It was time he did as well. After that bit of closure, he was fine about London. But from his wranglings with Ankrom, he wasn’t ready for Moscow. Time and energy that should have spent training and competing had gone into fighting the system that was supposed to be supporting him. By the autumn he had his mind made up he wasn’t going to compete in 2014.
He still works out every day: he either goes for a walk, a run or the gym out in Santry. He still coaches Laura and other walkers and is hugely conscious of what support structures – or lack of – might be out there for them. Laura is walking quicker times than Olive Loughnane and Gillian O’Sullivan were at her age.
They each won silver at the world championships. Yet she didn’t hear from Ankrom for over four months after the world championships. There is no head coach for walking in Ireland. Here is a sport where Ireland have won their last three world championship medals in. Without any real structure or culture in the event.
What would it be like if we had? “In this country, you have athletes who are trying to live like professionals. You have physios and sports scientists who are professional. But then all our coaches are voluntary. I know from coaching Laura there isn’t enough respect for coaches. There’s very little communication between the federation and the coaches.
Laura hadn’t heard from Kevin until the Monday after Christmas when he rang to tell her what her funding was for 2014. He’s supposed to be her performance manager. He hasn’t communicated with me – and I’m her coach. It turns out me and her physio and doctor sat down in September and outlined key areas such as injury prevention and strengthening her immune system, so we’ve been working away on that, and being proactive.
Other structures need to be put in place as well. The carding scheme he feels can sometimes inhibit an athlete as much as aid them. Sometimes you might need to take a step back to go two forward – Griffin himself would love to have broken down his faulty technique for a couple of years – but the need to get that next result to get the next bit of funding didn’t allow that. Less of a squeeze and more of a long-term investment plan would be better for everyone, he feels. As would a GPA-like representative body.
“If you talk to a lot of athletes they’ve often felt isolated and exposed and having to fend for themselves. At the moment athletes are just commodities. You’re only as good as your last race. You can be very easily disposed of. If you have one or two bad years you can go off the radar and be neglected. Then your career could be over at 30 and there’s nothing there to actually help you regarding advice on finance or career development and so on. Mental health is another area in a high-performance sport that hasn’t been looked at properly.
“You can get sucked into so many battles outside the track such as selection or funding with no one else able to represent you and energy you should be putting into your preparation and performance is being consumed elsewhere.”
These days a lot of his energy is going into developing a business (see altitudecentre.ie). Griffin has been fascinated by altitude training ever since 2007. He was training for his first 50km race so he trained at altitude in South Africa and upon his return availed of an altitude tent. A few months later in Slovakia, he won that first 50km race, setting a national record. He’d been able to train better, faster, for longer. He became so intrigued by this facility he visited the Altitude Centre in London and took on their Irish franchise. He made a proposal to University of Limerick to build Ireland’s first altitude house along the lines of the one at the Australian Institute of Sport. So they built and they have come, from international athletes to international rugby players to inter-county GAA players.
The next stage is to make his services more mainstream, less elitist. To have it just like your normal gym, only that bit more intense and challenging.
It’s a risk, this business, he knows, but then he’s coming from a sport where constantly left himself open to failure. Did he fail? It doesn’t sit well with him when people continuously remind him he’s an Olympian, something that can never be taken away from him.
“That doesn’t sit well with me at all. I don’t have a finishing performance to my name. I have to accept that for now. Do I have regrets? I didn’t do well enough at major championships. But I enjoyed my career. I still loved training, competing, learning. That has helped develop me as a coach probably more than as an athlete.”
It’s not that devoting so much to walking wasn’t worth it, so. It’s just that it’s not worth doing anymore – at least for now.”













 At the UPMC Sports Surgery Clinic, we individualise the lactate test to ensure it meets the athlete’s requirements, such as their current training status and the race distance they are preparing for. The lactate threshold and subsequent prescribed training programme for a 5km runner differ from that of a marathon runner.
At the UPMC Sports Surgery Clinic, we individualise the lactate test to ensure it meets the athlete’s requirements, such as their current training status and the race distance they are preparing for. The lactate threshold and subsequent prescribed training programme for a 5km runner differ from that of a marathon runner.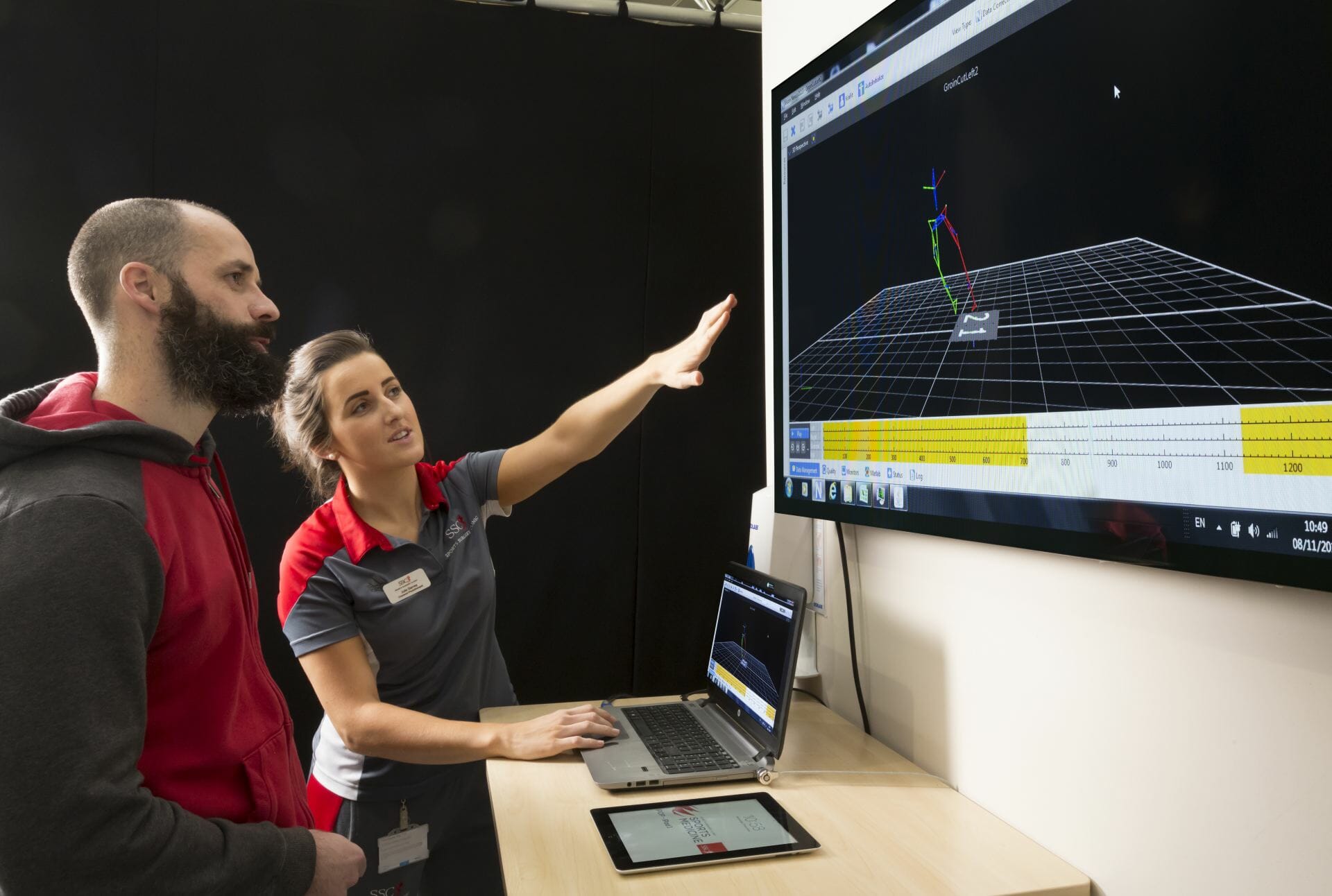
 New research by the UPMC Sports Surgery Clinic will help athletes and GAA players recover from the groin and hip injuries in nine weeks, according to
New research by the UPMC Sports Surgery Clinic will help athletes and GAA players recover from the groin and hip injuries in nine weeks, according to 











